Table 1: Grading Scheme for Acute Musculotendinous Strain Injury
Evaluation of Iliopsoas Strain with Findings from Diagnostic Musculoskeletal Ultrasound in Agility Performance Canines – 73 Cases
Robert E. Cullen DVM1
1Veterinary Orthopedic and Sports Medicine Group, 10975 Guilford Rd, Annapolis Junction, MD 20701
2Regenerative Orthopedics and Sports Medicine, 600 Pennsylvania Ave SE, Washington, DC 20003
*Corresponding Author (dcanapp@vosm.com)
Vol 2, Issue 2 (2017)
Published: 13 Jun 2017
Reviewed by: Wanda Gordon-Evans (DVM, PhD, DACVS) and Gillian Monsell (MA, VetMB, PhD, MRCVS)
DOI: 10.18849/VE.V2I2.93
Objective:
Iliopsoas injury and strain is a commonly diagnosed disease process, especially amongst working and sporting canines. There has been very little published literature regarding iliopsoas injuries and there is no information regarding the ultrasound evaluation of abnormal iliopsoas muscles. This manuscript is intended to describe the ultrasound findings in 73 canine agility athletes who had physical examination findings consistent with iliopsoas discomfort. The population was chosen given the high incidence of these animals for the development of iliopsoas injury; likely due to repetitive stress.
Methods:
Medical records of 73 agility performance canines that underwent musculoskeletal ultrasound evaluation of bilateral iliopsoas muscle groups were retrospectively reviewed. Data included signalment, previous radiographic findings, and ultrasound findings. A 3-tier grading scheme for acute strains was used while the practitioner also evaluated for evidence of chronic injury and bursitis.
Results:
The majority of pathologies were localised to the tendon of insertion, with the majority being low grade I-II strains (80.8%). Tendon fibre disruption (71.2%) and indistinct hypoechoic lesions (91.8%) were the most common of acute changes noted. Hyperechoic chronic changes were noted in 84.9 percent of cases. Acute and chronic changes were commonly seen together (62.8%).
Conclusion:
Diagnostic musculoskeletal ultrasound was used to identify lesions of the iliopsoas tendon consistent with acute and chronic injury, as well as identifying the region of pathology. The majority of agility performance dogs had low grade acute strains based on the tiered system, with mixed acute and chronic lesions being noted frequently.
Application:
Diagnostic musculoskeletal ultrasound provides a non-invasive diagnostic modality for patients suspected of having an iliopsoas strain.
Muscle strains are a commonly assessed injury amongst working and sporting animals.2,5,20 A previous survey with agility dogs found that thirty-two percent of the population had some degree of orthopaedic lameness during training, and that fifty-three percent of those evaluated by a veterinarian were due to muscle or tendon injury.5 The muscle is prone to acute strain from excessive stretch while engaged in eccentric contraction, wherein the external forces being driven across the muscle overload the contractile force of the muscle itself.3,4,23,28-29 The fibres of the muscle may then become disrupted and lose continuity, with additional disruption of the vascular supply leading to interstitial haemorrhage and swelling.28 Thirty-two percent of hind limb muscle strains in dogs involve the iliopsoas muscle group.6 Acute and chronic injury to the iliopsoas muscle groups has been a topic of interest in recent years with an increasing attention to diagnosis and treatment of this condition.
Clinical presentation with iliopsoas discomfort can include gait abnormalities and lameness with decreased coxofemoral extension. The lameness may be similar to patients with cranial cruciate ligament injury or hip dysplasia. When evaluating a patient with iliopsoas discomfort, a shortened stride with decreased hip extension is characteristic but not distinctive for iliopsoas in particular.2-3,20,22 Upon palpation there may be pain, spasm, and discomfort of the iliopsoas. Furthermore, many patients will be hesitant to allow coxofemoral extension with abduction and internal rotation as this specifically places stretch on the muscle and tendon in question.
An acute injury to the muscle or tendon has been characterised in 3 grades based on appearance during advanced imaging. Early human 3-tiered gradation structures have involved those based on clinical presentation33, but which have correlated well with later systems based on musculoskeletal ultrasound findings34,35, upon which we based our findings. Grade I strains have intact architecture and muscle function but with focal oedema or haemorrhage with less than 5%of the muscle involved. Such strains are generally the result of repeated muscle contractions resulting in mild muscle cell damage at the sarcomere. These injuries are rarely noted or diagnosed asides from athletic or performance animals, and generally resolve with appropriate rest in <1 week. Grade II strains have increased muscle involvement, mild fibre disruption, increased oedema or haemorrhage, and reduced strength of the musculotendinous unit. Grade III strains involve significant fascial tearing, muscle fibre disruption, and significant oedema or haemorrhage formation.2,33-35 (Table 1)
It is important to distinguish tendon strain and injury from muscle belly damage. The tendon unit primarily acts as a structure to transmit contractile force of the muscle. As such, they are often not rigid structures but have various degrees of elasticity and compliance. The general theorem of tendinous strain involves microtrauma and chronic overuse leading to a mechanical breakdown of the tendon. The lack of collagen support predisposes the structure to significant macroinjury. Gradation of tendon strains follows the same criteria and categories as that involving muscle trauma, differing only in the component of elastic recoil deformation. 8-9
The bursa is a tissue envelope surrounding the tendon of insertion as it approaches to and attaches to the lesser trochanter. This fluid-filled membrane allows for decreased friction between the tendon and bone. Bursitis, inflammation of the tissue membrane with resultant swelling and fluid collection, has been noted with other tendinous injuries. The bursa is collapsed in healthy patients, but can become enlarged and fluid distended in cases of acute or chronic injury.17-18,23-24 Acute and chronic bursitis inflammation can often be characterised, with acute injury showing as an anechoic fluid pocket and chronic injuries often having a thickened membrane and hyperechoic changes or debris within the space.31,32
Descriptions of imaging modalities for iliopsoas pathologies have been reported.11,14-17,19,23-26 Radiographs are unlikely to show evidence for iliopsoas strain, although they may detect mineralisation of the tendinous attachments, or enthesiophytosis, which has been seen with some instances of fibrotic myopathy and other chronic injuries.11 Computer tomography (CT) evaluation for acute iliopsoas strain has been previously described and found to be accurate for assessing intramuscular oedema and inflammation.14 Magnetic resonance imaging (MRI) has also been described for the assessment of iliopsoas injury in human and canine patients.15 However, these advanced imaging modalities are expensive to undertake, and require general anaesthesia. Due to expense and anaesthesia, it is also difficult to coordinate recheck evaluations to assess the injury following treatments.
Diagnostic musculoskeletal ultrasound evaluation has become a valuable and practical tool in assessing the iliopsoas and surrounding musculature. It is used frequently in human medicine for diagnostic evaluation of iliopsoas injuries, as well as for therapeutic injections.19, 23-24 While sedation is required for veterinary evaluation, full anaesthesia is not needed to perform an evaluation, which makes it of benefit over CT and MRI. It is also less expensive, making it a more viable option for both initial diagnostics and recheck examinations. Ultrasound evaluation of normal iliopsoas muscles was first reported in 2008 by Cannon and Puchalski where it was found that assessment of the whole iliopsoas muscle group could be performed using 8-5mHz curvilinear and 12-5mHz linear transducers with similar findings in cadaver specimens and live dogs.16 Additional ultrasound studies have been performed to identify the femoral nerve passage through the iliopsoas musculature.25-26 However, there have been few notations in literature regarding abnormalities of this muscle group using musculoskeletal ultrasound evaluation and no cataloguing of injury variety or severity.
The goal of this paper is to report the diagnostic musculoskeletal ultrasound findings of iliopsoas muscle strains in seventy-three canine athletes who had physical examination findings consistent with iliopsoas discomfort. The population was chosen given the high incidence of these animals for the development of iliopsoas injury.
Case Selection
Case records from January 2010 through July 2015 were analysed for agility dogs that underwent musculoskeletal ultrasound for iliopsoas discomfort assessed on physical examination (Veterinary Orthopedic Sports Medicine Group, Annapolis Junction, Maryland, USA). An assessment of iliopsoas injury on physical examination was found with dynamic evaluation, which involved placing the hip in extension and abduction and simultaneously internally rotating the stifle to evaluate for discomfort. All patients also experienced discomfort with direct palpation over the point of tendon insertion located cranial and deep to the pectineus muscle, at which point rigidity +/- spasm was appreciated. All cases in this paper were recommended to have musculoskeletal ultrasound performed in order to identify lesions and facilitate a recommended treatment protocol. Documentation of, and treatment for, co-morbidities (cruciate injury, hip dysplasia, lumbar discomfort, etc.) was not taken into account as this paper was intended to document musculoskeletal ultrasound findings for patients with physical examination findings consistent with an iliopsoas injury as either primary disease or secondary.
Evaluation of the Iliopsoas Using Ultrasound
During ultrasound, sedation was always performed to allow for a thorough evaluation of the structures. This was both due to discomfort from pressure from the transducer over inflamed muscle tendons and fibres, but also to facilitate dorsal recumbency and relaxation to obtain the best views. Patients were sedated with dexmedetomidine 0.03mg/kg and butorphanol 0.2mg/kg IV or IM prior to evaluation. Ultrasound was performed using a Hitachi-Aloka Noblus system with an 18mHz probe. All examinations were performed by a single experienced practitioner (DC).
When approaching musculoskeletal ultrasound of the iliopsoas groups, the anatomy was loosely grouped into three regions: insertion, muscle belly, and origin, and the assessments are made in that order. Acute injury would result in swelling, oedema, inflammation, and possibly haemorrhage. Such changes would be evident on ultrasound based on enlargement of muscle fibres (swelling, inflammation) and a distinctly demarcated hypoechoic region (oedema, haemorrhage). Such demarcated hypoechoic lesions were classified as “core lesions”. Identification and characterisation of acute muscle and tendon injuries were done so using a Grade I-III scheme. A grade of I-II or II-III was given to those cases with components of injury reserved for two different grade classes. For example, a case with signs of mild bruising and very mild fascial tearing may be given a Grade of I-II. (Table 1)
The musculoekeltal ultrasound evaluation was started with the probe placed cranial to the pectineus and parallel to the femur. This view allows for a general approach to the location to assess the anatomy. However, it results in obliquity of the tendon fibres, with variation on characterisation based on the patient. A more standardised view involves a caudal longitudinal evaluation of the insertion. (Figure 1a) A more detailed image of the lesser trochanter and bursa is made from this angle. A transverse view across the femur from the caudal aspect is also of importance when evaluating the insertion tendon. (Figure 1b) The tendon is seen as a short, linear, hyperechoic structure attaching to a small shadowing protrusion of the medial femur (the lesser trochanter). Evaluation was made for fibre tears, bursitis, core lesions, or evidence of chronic fibrosis. Following the muscle group, the myotendinous junction (MTJ) was evaluated with the probe facing slightly cranial. (Figure 1c) The MTJ is seen as a fan-shaped structure that is generally hypoechoic with obliquely oriented hyperechoic strands.
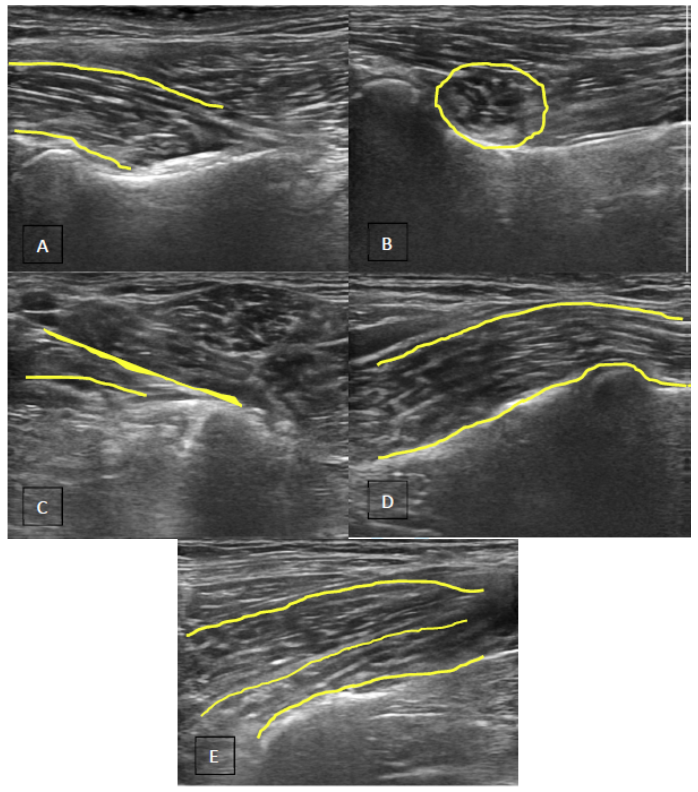
The muscle belly is found ventral to the lumbar vertebral bodies four through seven. Normal muscle tissue is noted to have a generalised homogenous hypoechoic parenchyma with linear lines of hyperechoic muscle fibres obliquely oriented. Differentiation of the iliacus muscle from the psoas major muscle is visualised over the ischium (Figure 1d). The iliacus can then sometimes be traced back to its origin on the ilium (Figure 1e). The femoral nerve can be found between the major psoas and iliacus muscle bellies.
The psoas major origin is identified by tracing the muscle belly proximally to the transverse processes of the third lumbar veterbrae and observing the hypoechoic attachments with linear hyperechoic fibres oriented obliquely. The L3 origin can often be appreciated in smaller dogs (less than 50 pounds). The origin was often obscured in larger animals with large amounts of muscle or fat, and may also be obscured by gas shadowing from the colon.
Signalment
Seventy-three dogs underwent diagnostic musculoskeletal ultrasound for suspected iliopsoas injury assessed on physical examination from January 2010 through July 2015. Physical examinations on all canines evaluated included hind limb lameness (unilateral or bilateral), with discomfort on extension and internal rotation of the noted hind limb, and with rigidity +/- spasm and discomfort on direct palpation of the iliopsoas muscle belly or tendon. Mean age at the time of initial examination was 5.1 years (median 5.0 years, range 2 to 10 years). 54.8 percent were female (32 spayed, 8 intact), and 45.2 percent were male (20 neutered, 13 intact). Excluding mixed breed canines, twenty-two breeds were evaluated. The most common breeds were Border Collies (27.4%), Australian Shepherds (11%), Shetland Shepherds (6.8%), and Welsh Corgis (5.5%). Mean body weight was 44.15 pounds (20.07kg) with a median body weight of 42.4 pounds (19.27kg) and a range of 10 to 86.7 pounds (4.55-39.4kg).
Non-Ultrasonic Imaging
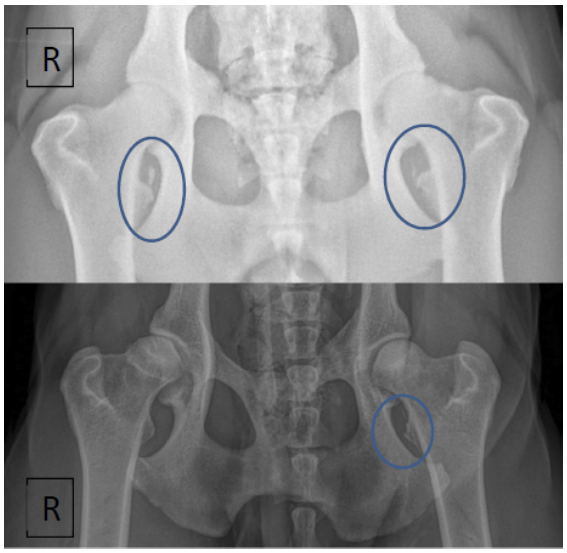
Of 73 cases, 59 had pelvis radiographs performed. Of these, tendinous calcification (enthesiophytosis), an indication of severe chronic muscle tendon inflammation, was noted in four patients. Mild remodeling changes to the lesser trochanter were noted in an additional five cases. (Figure 2) Five cases were also noted to have coxofemoral degenerative changes consistent with dysplasia or osteoarthritis.
For our case population, there were eight MRI reports available of the lumbosacral from board-certified radiologists to assess for vertebral and pelvic pathology (Phillip Gyroscan 1.5 Tesla Unit). Five of these reports reported normal iliopsoas on MRI with no apparent abnormalities. Based on interpretation of ultrasound evaluation, three of these five cases had chronic changes, one had mild bursitis, and three had mild Grade I-II strains of the tendon. Two of the eight MRI reports made no mention of the iliopsoas muscle group. Both of these cases had chronic changes noted on ultrasound, and one was found to have a significant Grade II-III muscle strain. One MRI report of the eight made mention of hyperintense streaks of the body and insertion unilaterally, which was noted as a mild Grade I strain on ultrasound evaluation. No CT evaluations of the pelvis were made for this case series.
Musculoskeletal Ultrasound
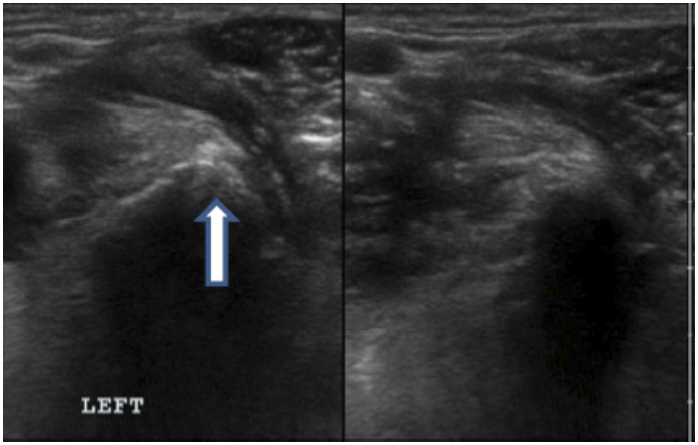
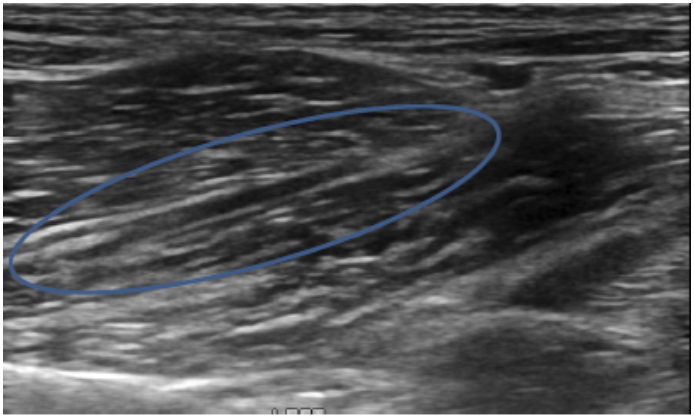
Figures 3-6 show gradations of hypoechoic lesions and fascial tearing using in the tiered grading system for muscular or tendinous injuries. A distinctly demarcated “core” lesion is noted in Figure 3.
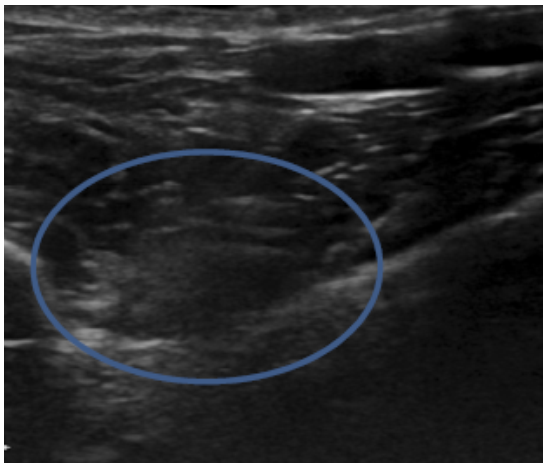
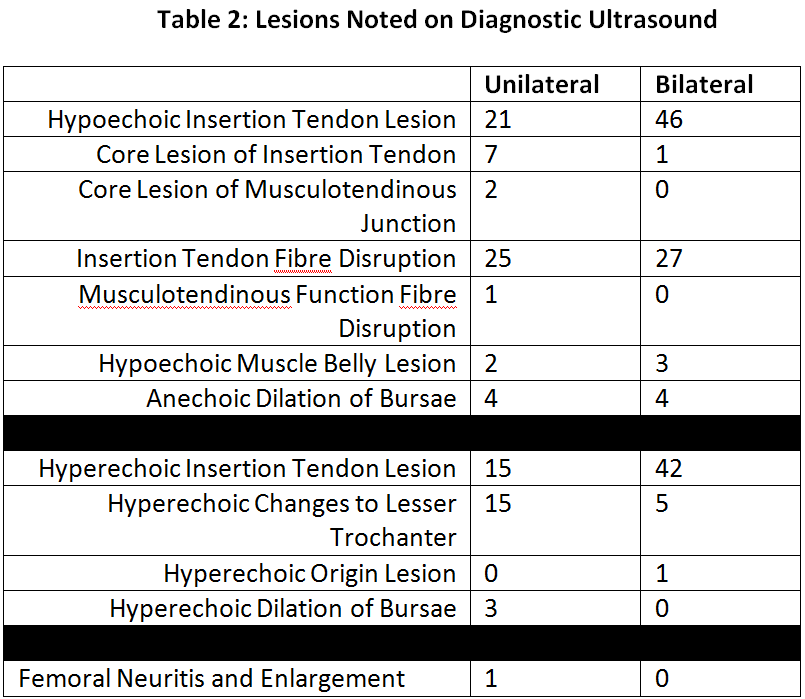
Hypoechoic changes of the tendon of insertion were noted in 91.8 percent of cases (21 unilateral, 46 bilateral). Various degrees of insertion tendon fibre disruption were seen in 71.2 percent of cases (25 unilateral, 27 bilateral). Distinct hypoechoic core lesions were noted in 11 percent of cases (7 unilateral, 1 bilateral). Lesions of the musculotendinous junction were noted in 4.1 percent of cases (2 core lesions, 1 case with fibre disruption). Hypoechoic changes to the muscle belly were noted in 6.8 percent of cases (2 unilateral, 3 bilateral). No changes to the origins of the iliopsoas muscles were noted. (Table 2)
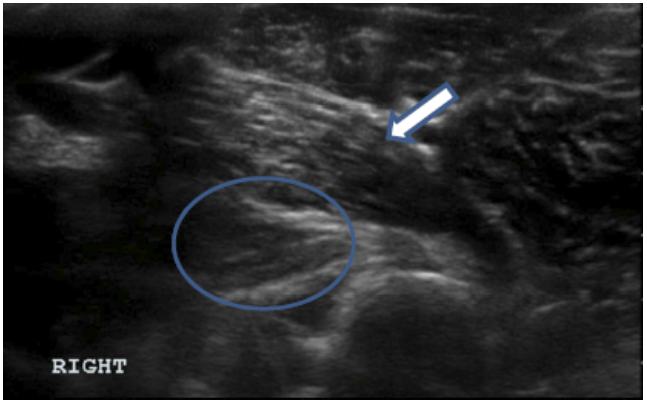
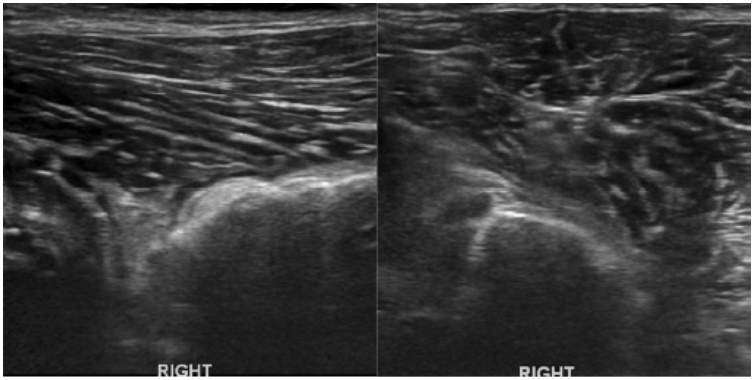
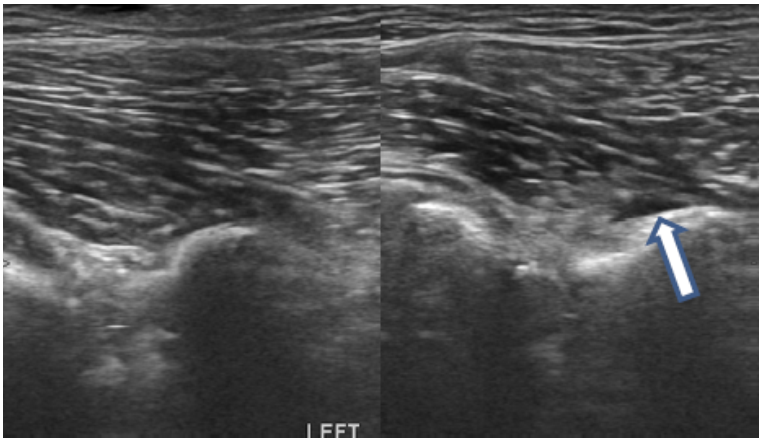
Frequently noted were various hyperechoic abnormalities within the muscle belly or tendon of insertion that did not align with typical hyperechoic fibres of the iliopsoas muscular unit. Enthesiophytes and remodeling changes of the lesser trochanter were also distinctly noted as hyperechoic and shadowing.1,2,16,27. (Figure 7)
Hyperechoic fibres of the insertion tendon in 78.1 percent of cases (15 unilateral, 42 bilateral) and hyperechoic periosteal changes to the lesser trochanter in 27.4 percent of cases (15 unilateral, 5 bilateral). It is important to note that in only 5.5 percent of cases were lesser trochanter changes noted on radiographs. In one case, hyperechoic changes at the origin of the major psoas muscle bilaterally were noted. (Table 2)
It was not uncommon to see a mixture of lesions (hypoechoic +/- fibre disruption and hyperechoic). For our case selection, 66.2 percent of cases with ultrasound findings of hypoechoic lesions +/- fibre disruption were also found with hyperechoic lesions, as well.
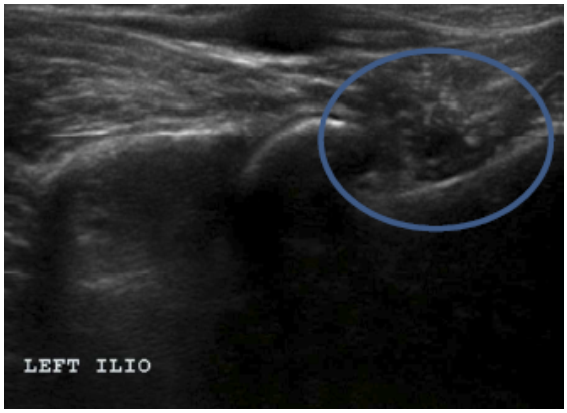
In one patient, inflammation of the femoral nerve, which supplies and runs between the major psoas and ilacus muscles, was noted during evaluation of the iliacus and psoas major muscle bellies. (Figure 8)
The bursa was also examined during the musculoskeletal ultrasound evaluation. Eleven cases (15.1 percent) had evidence of inflammation and fluid dilation within the bursa. Of these, three (27.3 percent) showed to have mildly hyperechoic fluid (all unilateral). The remaining eight cases (72.7 percent) showed anechoic fluid distension (4 unilateral, 4 bilateral). (Figure 9)
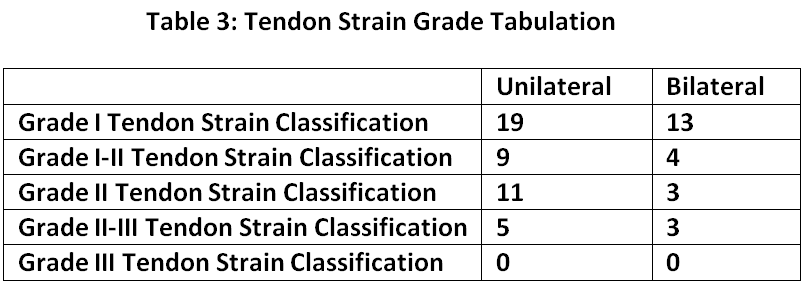
When evaluating the findings from our case selection, musculoskeletal ultrasound found 6.8 percent (2 unilateral, 3 bilateral) with only hyperechoic changes. When using our tiered gradation system for hypoechoic and fibre disruption lesions, the results returned with 43.8 percent (19 unilateral, 13 bilateral) with Grade I strain, 17.8 percent (9 unilateral, 4 bilateral) with Grade I-II strain, 19.2 percent (11 unilateral, 3 bilateral) with Grade II strain, and 11 percent (5 unilateral, 3 bilateral) with Grade II-III strain. Imaging showing complete Grade III strain was not found in our case selection. These final numbers are based on the most severe lesions seen on ultrasound, whether bilateral and unilateral, and do not account for lesser changes seen on the contralateral iliopsoas for those assessed with a unilateral condition. (Table 3)
Diagnostic musculoskeletal ultrasound is utilised frequently in human orthopaedic and sports medicine as a means to identify injury, differentiate acute and chronic injury, and facilitate treatment protocols. This tool is frequently used in our facility to the same ends. To our knowledge, this is the first paper documenting lesions in a case series of the iliopsoas muscle using musculoskeletal ultrasound.
We have used ultrasound assessment to identify lesions consistent with acute and chronic iliopsoas strains, with distinct characteristics associated with each grade of pathology that can be assessed. Full assessment of the iliopsoas muscle with ultrasound takes time and practice to perform, but is often instrumental for the diagnostic process in nebulous hind limb lameness.
The findings of hypoechoic lesions of the belly or tendon of a muscle are being interpreted as acute injury, and the result of oedema or haemorrhage within the muscle unit. Fibre disruption was also noted with presumed acute injuries and was utilised in the tiered grading system along with severity of hypoechoic lesions in determining grade of the injury. While fibre disruption may be noted in chronic injuries, it was more typically noted as hyperechoic scar tissue or fibrosis, presumably from a previous acute strain.
Iliopsoas discomfort can present to clinicians as acute injury or the result of a chronic strain. Chronic iliopsoas pain is often seen with, and presumed the result of long-term compensation for, a chronic primary hip, stifle, or lumbar spine pathology. The joint is protected by limiting its range of motion in abduction and rotation. Such restriction puts additional burden on the hip stabilisers to maintain gait, resulting in chronic fatigue, decreasing muscle fibre elasticity, and can predispose the muscle group to cycles of local inflammation and strain.2,10,23,28-30 In the event of mild Grade I strains, there is typically preservation of connective sheaths and sarcolemal cells that allows for complete regeneration of the fibres with proper activity restrictions. However, if extensive disruption and haemorrhage occur, or if acute injuries are not rested appropriately, a cycle of contracture and fibroplasia can be the result. Fibroplasia from scar tissue formation provides stability but may prevent proper spread of myofibrils, inhibiting proper healing.2,10,29 Scar tissue will inhibit normal muscular contraction and relaxation, resulting in chronic mechanical lameness from fibrotic contracture. 10, 29-30 In these injuries, chronic damage would be prone to repeated acute re-injury, which would explain the large number of cases with mixed (acute and chronic) changes noted on ultrasound.
The accumulation of scar tissue from chronic injury can lead to an irreversible fibrotic myopathy, which has been described as necessitating a tenomyectomy procedure to alleviate clinical signs.7,11-13,29 Given the proximity of the femoral nerve to the iliopsoas group, a further uncommon but reported sequelae is femoral nerve dysfunction resulting from iliacus compartment syndrome. This would present as pain, decreased patellar and withdrawal reflexes, and possibly decreased superficial medial limb sensation.2,6-7,12,29 Femoral neuritis and enlargement was noted in one patient from our case population. Given the lack of case numbers with this finding, it is difficult to make any further comment on this finding, but it worth consideration during evaluation of the iliopsoas muscle group as potential sequelae.
Bursitis was noted in eleven patients in this case series, with three and eight of the cases showing changes consistent with chronic and acute bursae inflammation, respectively. Those three cases with mildly hyperechoic changes also demonstrated chronic changes of the iliopsoas tendon, and all eight cases showing anechoic fluid dilation also demonstrated acute injury to the iliopsoas tendon.
The majority of lesions noted on ultrasound in our case population, both acute and chronic, were localised to the tendon of insertion. The tendon unit primarily acts as a structure to transmit contractile force of the muscle. As such, they are often not rigid structures but have various degrees of elasticity and compliance. The recoil action of certain tendons once loads are released in the form of passive energy can be important in preserving energy during locomotion. Various loads held for various times or repetitions will alter this elasticity.8-9 In vitro testing of tendinous structures at increasing loads have found tendons to continuously elongate with aligned fibres until eventual end-point failure and breakage with increasing deformation and decreased elastic recoil potential over time due to a breakdown of collagen fibre crosslinking.9 The general theorem of tendinous strain involves microtrauma and chronic overuse leading to a mechanical breakdown of the tendon. The lack of collagen support predisposes the structure to significant macroinjury. Gradation of tendon strains follows the same criteria and categories as that involving muscle trauma, differing only in the component of elastic recoil deformation. 8-9
The MRI report findings demonstrated consistently inferior evaluation of the iliopsoas muscle group compared to diagnostic musculoskeletal ultrasound findings. MRI failed to identify mild strains and chronic injury, as well as one instance of a Grade II-III strain. It should be noted that the majority of these cases were undergoing MRI to evaluate for lumbosacral pathology, rather than an evaluation of the iliopsoas, and so while the iliopsoas was within the field of view and was commented upon in several reports, the ideal parameters for evaluating the iliopsoas were not used for these studies and so comparison between the different imaging modalities is not possible for our case selection. Further studies comparing the two modalities are warranted.
An important limitation of this presentation is case selection. The ultrasound and physical examination findings show a fairly high percentage of moderate to high-grade iliopsoas sprains (Grades II or higher). Also, no Grade III lesions were present in this case series. Even so, in the authors’ experience, this is not an accurate assessment of the general population of iliopsoas strains. Most of the cases assessed with ultrasound in this case series were presenting with significant acute or prolonged chronic discomfort, and often after a long history of activity restriction, anti-inflammatory and muscle relaxant medications, and various modalities of rehabilitation therapy prior to ultrasound evaluation. However, in the authors’ experience, the majority of iliopsoas strains presenting for evaluation with discomfort on iliopsoas palpation (of both athletic and companion animals) are mild Grade I injuries which likely improve with rehabilitation therapy and medical management. In addition, our case selection consisted entirely of agility performance animals with excellent body condition and highly athletic lifestyles that is unlikely to be the norm for most companion animals.
It is also important to note that the majority of cases presenting with iliopsoas discomfort often do so after a long history of nebulous hind limb lameness, with only rarely a distinct traumatic event initiating a diagnostic work-up. As such, the findings of acute vs chronic musculoskeletal changes on ultrasound must be interpreted with the understanding that these injuries are often cyclical, with repeated bouts of acute injury re-presenting with a slow accumulation of hyperechoic chronic changes. As such, while a clear timeline from time of first injury until presentation would be ideal, it is not always possible.
Another important limitation in this case series would be the lack of histologic testing to correlate with musculoskeletal ultrasound findings. So while distinct and differing changes to the muscle unit were noted, the assessment of these being acute or chronic (or mixed) injuries was done so by clinician interpretation based on experience and previous studies.
The involvement of comorbidities is an important one to consider with evaluation of muscle strain injuries, especially of the iliopsoas muscle group. Primary muscle injury as a result of rapid turns and twists inherent in a sporting dog’s lifestyle would be more likely than the typical routine of a companion animal. However, in the authors’ experience, ongoing muscle fatigue and microtrauma secondary to compensation from an underlying orthopaedic injury (stifle, hip, or lumbar) is an important consideration. This paper was intended to document lesions from musculoskeletal ultrasound evaluation following identification of iliopsoas discomfort on physical examination in canine agility athletes, and so an accounting of previous or subsequent comorbidities was beyond the intention or scope of this paper. However, further study in the correlation of treatment protocols following iliopsoas strain identification with repeat musculoskeletal ultrasound and lameness outcomes, while taking into account potential underlying or concurrent morbidities, is warranted.
There has been no previous in-depth evaluation or description of diagnostic musculoskeletal ultrasound findings of iliopsoas muscle strains. This paper describes the most common lesions and findings associated with strains. Appreciation of the severity of lesions can potentially be correlated with the degree of lameness but also play a role when deciding treatment strategies. Further study on the utility of ultrasound assessment, especially in regard to monitoring of lesions through various treatment protocols and recovery process, is warranted. Ultrasound re-evaluations can potentially be key component in assessing for structural integrity of the iliopsoas muscle and tendon during the treatment process.
Funding: No outside funding or grants were used for this research paper.
Competing interests: There are no competing financial interests or conflicts of interests involved with the production of this research paper.
Intellectual Property Rights
Authors of articles submitted to RCVS Knowledge for publication will retain copyright in their work, but will be required to grant to RCVS Knowledge an exclusive licence of the rights of copyright in the materials including but not limited to the right to publish, re-publish, transmit, sell, distribute and otherwise use the materials in all languages and all media throughout the world, and to licence or permit others to do so.
Authors will be required to complete a licence for publication form, and will in return retain certain rights as detailed on the form.